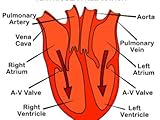
left ventricular preload - click on the image below for more information. 
left ventricular preload
A complete, hands-on guide to successful image acquisition and interpretation at the bedside "The real strength of this textbook is its clinical focus. The editors are to be complimented on keeping a consistent structure within each chapter, beginning with basic physical principles, practical "knobology," scanning tips, key findings, pitfalls and limitations, and how the key findings relate to bedside patho-physiology and decision-making. Thus, the authors have succeeded in providing
Critical Care Ultrasonography (with DVD)
Click on the button for more left ventricular preload information and reviews.
Slide2Call - Stop Accidental Dialing Slide2Call is a mobile application that prevents you from making unwanted accidental calls. Each attempt to make a call is interrupted by a ready-to-confirm slider. To proceed with the call, simply move the slider from left to right. For Windows Mobile!
Slide2Call - Stop Accidental Dialing Angiotensin Article by jekky
Precursor, and types of angiotensin AngiotensinogenAngiotensinogen is an -2-globulin that is produced constitutively and released into the circulation mainly by the liver. It is a member of the serpin family, although it is not known to inhibit other enzymes, unlike most serpins. Plasma angiotensinogen levels are increased by plasma corticosteroid, estrogen, thyroid hormone, and angiotensin II levels.Angiotensinogen is also known as renin substrate.Human angiotensinogen is 452 amino acids long, but other species have angiotensinogen of varying sizes. The first 12 amino acids are the most important for activity.Asp-Arg-Val-Tyr-Ile-His-Pro-Phe-His-Leu-Val-Ile Angiotensin IAsp-Arg-Val-Tyr-Ile-His-Pro-Phe-His-LeuRenin-angiotensin-aldosterone systemAngiotensin I (CAS# 11128-99-7) is formed by the action of renin on angiotensinogen. Renin is produced in the kidneys in response to both decreased intra-renal blood pressure at the juxtaglomerular cells, or decreased delivery of Na+ and Cl- to the macula densa. If more Na+ is sensed, renin release is decreased.Renin cleaves the peptide bond between the leucine (Leu) and valine (Val) residues on angiotensinogen, creating the ten amino acid peptide (des-Asp) angiotensin I (CAS# 9041-90-1).Angiotensin I appears to have no biological activity and exists solely as a precursor to angiotensin 2. Angiotensin IIAsp-Arg-Val-Tyr-Ile-His-Pro-PheAngiotensin I is converted to angiotensin II through removal of two C-terminal residues by the enzyme angiotensin-converting enzyme (ACE, or kinase), which is found predominantly in the capillaries of the lung. ACE is actually found all over the body, but has its highest density in the lung due to the high density of capillary beds there. Angiotensin II acts as an endocrine, autocrine/paracrine, and intracrine hormone.ACE is a target for inactivation by ACE inhibitor drugs, which decrease the rate of angiotensin II production. Angiotensin II increases blood pressure by stimulating the Gq protein in vascular smooth muscle cells (which in turn activates contraction by an IP3-dependent mechanism). ACE inhibitor drugs are major drugs against hypertension.Other cleavage products of ACE, 7 or 9 amino acids long, are also known; they have differential affinity for angiotensin receptors, although their exact role is still unclear. The action of angiotensin II itself is targeted by angiotensin II receptor antagonists, which directly block angiotensin II AT1 receptors.Angiotensin II is degraded to angiotensin III by angiotensinases that are located in red blood cells and the vascular beds of most tissues. It has a half-life in circulation of around 30 seconds, whereas, in tissue, it may be as long as 1530 minutes. Angiotensin IIIAsp | Arg-Val-Tyr-Ile-His-Pro-PheAngiotensin III has 40% of the pressor activity of Angiotensin II, but 100% of the aldosterone-producing activity. Angiotensin IVArg | Val-Tyr-Ile-His-Pro-PheAngiotensin IV is a hexapeptide that, like angiotensin III, has some lesser activity. EffectsSee also Renin-angiotensin_system#EffectsAngiotensins II, III & IV have a number of effects throughout the body: Cardiovascular effectsThey are potent direct vasoconstrictors, constricting arteries and veins and increasing blood pressure.Angiotensin II has prothrombotic potential through adhesion and aggregation of platelets and production of PAI-1 and PAI-2.When cardiac cell growth is stimulated, a local (autocrine-paracrine) renin-angiotensin system is activated in the cardiac myocyte, which stimulates cardiac cell growth through Protein Kinase C. The same system can be activated in smooth muscle cells in conditions of hypertension, atherosclerosis, or endothelial damage. Angiotensin II is the most important Gq stimulator of the heart during hypertrophy, compared to endothelin-1 and A1 adrenoreceptors. Neural effectsAngiotensin III increases thirst sensation (dipsogen) through the subfornical organ (SFO) of the brain, decreases the response of the baroreceptor reflex, and increases the desire for salt. It increases secretion of ADH in the posterior pituitary and secretion of ACTH in the anterior pituitary. It also potentiates the release of norepinephrine by direct action on postganglionic sympathetic fibers. Adrenal effectsAngiotensin II acts on the adrenal cortex, causing it to release aldosterone, a hormone that causes the kidneys to retain sodium and lose potassium. Elevated plasma angiotensin II levels are responsible for the elevated aldosterone levels present during the luteal phase of the menstrual cycle. Renal effectsAngiotensin II has a direct effect on the proximal tubules to increase Na+ reabsorption. It has a complex and variable effect on glomerular filtration and renal blood flow depending on the setting. Increases in systemic blood pressure will maintain renal perfusion pressure, however constriction of the afferent and efferent glomerular arterioles will tend to restrict renal blood flow. The effect on the efferent arteriolar resistance is, however, markedly greater, in part due to its smaller basal diameter; this tends to increase glomerular capillary hydrostatic pressure and maintain glomerular filtration rate. A number of other mechanisms can affect renal blood flow and GFR. High concentrations of Angiotensin II can constrict the glomerular mesangium reducing the area for glomerular filtration. Angiotensin II as a sensitizer to tubuloglomerular feedback preventing an excessive rise in GFR. Angiotensin II causes the local release of prostaglandins, which, in turn, antagonize renal vasoconstriction. The net effect of these competing mechanisms on glomerular filtration will vary with the physiological and pharmacological environment.Renal effects of Angiotensin IITargetActionMechanismRenal artery &afferent arteriolesvasoconstrictionVDCCs Ca2+ influxefferent arteriolevasoconstriction(probably) activate Angiotensin receptor 1 Activation of Gq LC activity P3 and DAG activation of IP3 receptor in SR ntracellular Ca2+mesangial cellscontraction iltration areaactivation of Gq LC activity P3 and DAG activation of IP3 receptor in SR ntracellular Ca2+VDCCs Ca2+ influxTubuloglomerular feedbackIncreased sensitivityIncrease in afferent arteriole responsiveness to signals from macula densamedullary blood flowReduction See alsoACE inhibitorAngiotensin receptorAngiotensin II receptor antagonist References^ Basso N, Terragno NA (December 2001). "History about the discovery of the renin-angiotensin system". Hypertension 38 (6): 12469. doi:10.1161/hy1201.101214. PMID 11751697. http://hyper.ahajournals.org/cgi/pmidlookup?view=long&pmid=11751697. ^ NCBI HomePage^ Physiology at MCG 7/7ch09/7ch09p16^ Skurk T, Lee YM, Hauner H (May 2001). "Angiotensin II and its metabolites stimulate PAI-1 protein release from human adipocytes in primary culture". Hypertension 37 (5): 133640. PMID 11358950. http://hyper.ahajournals.org/cgi/pmidlookup?view=long&pmid=11358950. ^ Gesualdo L, Ranieri E, Monno R, et al. (August 1999). "Angiotensin IV stimulates plasminogen activator inhibitor-1 expression in proximal tubular epithelial cells". Kidney Int. 56 (2): 46170. doi:10.1046/j.1523-1755.1999.00578.x. PMID 10432384. ^ Unless else specified in table, then ref is: Walter F., PhD. Boron (2005). Medical Physiology: A Cellular And Molecular Approaoch. Elsevier/Saunders. ISBN 1-4160-2328-3. Page 771 Further readingde Gasparo M, Catt KJ, Inagami T, "et al." (2000). "International union of pharmacology. XXIII. The angiotensin II receptors". Parmacol Rev. 52: 415472. PMID 10977869. Brenner & Rector's The Kidney, 7th ed., Saunders, 2004.Mosby's Medical Dictionary, 3rd Ed., CV Mosby Company, 1990.Review of Medical Physiology, 20th Ed., William F. Ganong, McGraw-Hill, 2001.Clinical Physiology of Acid-Base and Electrolyte Disorders, 5th ed., Burton David Rose & Theodore W. Post McGraw-Hill, 2001Lees KR, MacFadyen RJ, Doig JK, Reid JL (1993). "Role of angiotensin in the extravascular system". Journal of human hypertension 7 Suppl 2: S712. PMID 8230088. Weir MR, Dzau VJ (2000). "The renin-angiotensin-aldosterone system: a specific target for hypertension management". Am. J. Hypertens. 12 (12 Pt 3): 205S213S. doi:10.1016/S0895-7061(99)00103-X. PMID 10619573. Berry C, Touyz R, Dominiczak AF, et al. (2002). "Angiotensin receptors: signaling, vascular pathophysiology, and interactions with ceramide". Am. J. Physiol. Heart Circ. Physiol. 281 (6): H233765. PMID 11709400. Sernia C (2002). "A critical appraisal of the intrinsic pancreatic angiotensin-generating system". JOP 2 (1): 505. PMID 11862023. Varagic J, Frohlich ED (2003). "Local cardiac renin-angiotensin system: hypertension and cardiac failure". J. Mol. Cell. Cardiol. 34 (11): 143542. doi:10.1006/jmcc.2002.2075. PMID 12431442. Wolf G (2006). "Role of reactive oxygen species in angiotensin II-mediated renal growth, differentiation, and apoptosis". Antioxid. Redox Signal. 7 (9-10): 133745. doi:10.1089/ars.2005.7.1337. PMID 16115039. Cazaubon S, Deshayes F, Couraud PO, Nahmias C (2006). "[Endothelin-1, angiotensin II and cancer]". Med Sci (Paris) 22 (4): 41622. PMID 16597412. Ariza AC, Bobadilla NA, Halhali A (2007). "[Endothelin 1 and angiotensin II in preeeclampsia]". Rev. Invest. Clin. 59 (1): 4856. PMID 17569300. ... External linksMeSH Angiotensinsv d eCardiovascular system, physiology: cardiovascular physiologyHeartVolumesStroke volume = End-diastolic volume End-systolic volumeCardiac output = Heart rate Stroke volumeAfterload PreloadFrank-Starling law of the heart Cardiac function curve Venous return curveAortic valve area calculation Ejection fraction Cardiac indexInteraction diagramsCardiac cycle Wiggers diagram Pressure volume diagramTropismChronotropic (Heart rate) Dromotropic (Conduction velocity) Inotropic (Contractility) Batmotropic (Excitability) Lusitropic (Relaxation)Conduction system /Cardiac electrophysiologyCardiac action potential (Atrial action potential, Ventricular action potential) Effective refractory period Pacemaker potential EKG (P wave, PR interval, QRS complex, QT interval, ST segment, T wave, U wave) Hexaxial reference systemChamber pressureCentral venous pressure/right atrial pressure Right ventricular pressure Pulmonary artery pressure Pulmonary wedge pressure/left atrial pressure Left ventricular pressure Aortic pressureOtherVentricular remodelingVascular system/HemodynamicsBlood flowCompliance Vascular resistance (Total peripheral resistance) Pulse PerfusionBlood pressurePulse pressure (Systolic - Diastolic) Mean arterial pressureJugular venous pressurePortal venous pressureRegulation of BPBaroreflex Kinin-kallikrein system Renin-angiotensin system Vasoconstrictors/Vasodilators Autoregulation (Myogenic mechanism, Tubuloglomerular feedback) Paraganglia (Aortic body, Carotid body, Glomus cell)heart navs: anat/physio/dev, noncongen/congen/neoplasia, symptoms+signs/eponymous, procvascular navs: anat/physio/dev, noncongen/systemic vasculitis/congen/neoplasia, symptoms+signs/eponymous, procv d ePeptides: neuropeptidesHypothalamicSomatostatin CRH GnRH GHRH Orexins TRH POMC (ACTH MSH Lipotropin)Gastrointestinal hormonesCholecystokinin Gastric inhibitory polypeptide Gastrin Motilin Secretin Vasoactive intestinal peptideOther hormonesCalcitonin Oxytocin VasopressinOther neuropeptidesAngiotensin Bombesin Calcitonin gene-related peptide Carnosine Cocaine and amphetamine regulated transcript Delta sleep-inducing peptide FMRFamide Galanin Galanin-like peptide Gastrin releasing peptide Kinins (Bradykinin Tachykinins) Neuropeptide S Neuropeptide Y Neurophysins Neurotensin Pancreatic polypeptide Pituitary adenylate cyclase activating peptide VGFNeuromedinsB N S UOpioid peptidesDynorphin Endomorphin Endorphin Enkephalin Nociceptin Opiorphinv d eAutacoidsKininsKininogen (HMWK, LMWK) Bradykinin Kallidin Tachykinins Urotensin-IIOthersAngiotensin Eicosanoid Histamine Platelet-activating factor Serotonin Categories: Human proteins | Peptide hormones | Cardiovascular system | Endocrinology | Physiology
About the Author
I am an expert from Components Electronic suppliers, usually analyzes all kind of industries situation, such as airsoft thompson, skin care private label.
Orignal From:
Critical Care Ultrasonography (with DVD)